
Designing a scalable mobile based strategy for women from disadvantaged families to navigate the healthcare system during ‘First 1000 Days’ from conception through to 2 years old.
This project, undertaken as part of the Master of Design Futures program, Future Design Clients unit, focused on empathetically engaging with the experience of a child and family in the ‘First 1000 Days’ from conception through to 2 years old (this period is roughly 1000 days — from pregnancy confirmation to the time when the child is 2 years). It’s a crucial period in the woman’s as well as the child’s life as it has a lifetime impact on their respective healths. The aim was to find out how design can help disadvantaged families to navigate the healthcare system. We were encouraged to go beyond what is expected from a ‘work’ project and instead to creatively craft approaches to grow the practice.
Defining the territory
We were asked to choose one of four personas derived from the lived experiences of a family in Melbourne’s West. I crafted the persona of a lady — Suman, that was relevant to Mumbai.

I wrote a story about Suman’s life story to date. This exercise helped me fill in the gaps in her story and justify her life choices. It was important to visually represent her personal history to highlight positive and negative moments. A story-telling exercise could aid other stakeholders in empathising with her as well.

The area I chose was the Slums of Behram Baug in Mumbai. It is a slum township in itself with over 400,000 people living in poorly constructed illegal shanties. I then started mapping out the first, second, third places and allied services. The woman’s surroundings, support systems, engagement points and third places play an important role in defining her experience of the first 1000 days. Three types of network maps were created to represent the services available to her, the ones she uses and her immediate surroundings which affect her well-being. She may not use all the services due to lack of awareness, time, need or money.

Available services within 3 km

Services used by Suman

Zoomed-in view of the slums of Behram Baug
Relationship mapping
This was a diagrammatic representation of her experiences and her relationships that are pivotal to her and her family having positive health outcomes. A visual depiction helped zoom in on one aspect of the persona — either in the form of the services she gets, her family or people in the surroundings. This exercise further helped narrow down on her problem area and communicating her emotional experiences. It was particularly challenging since it needed some extrapolation and imagination based on observation, reading and logic.
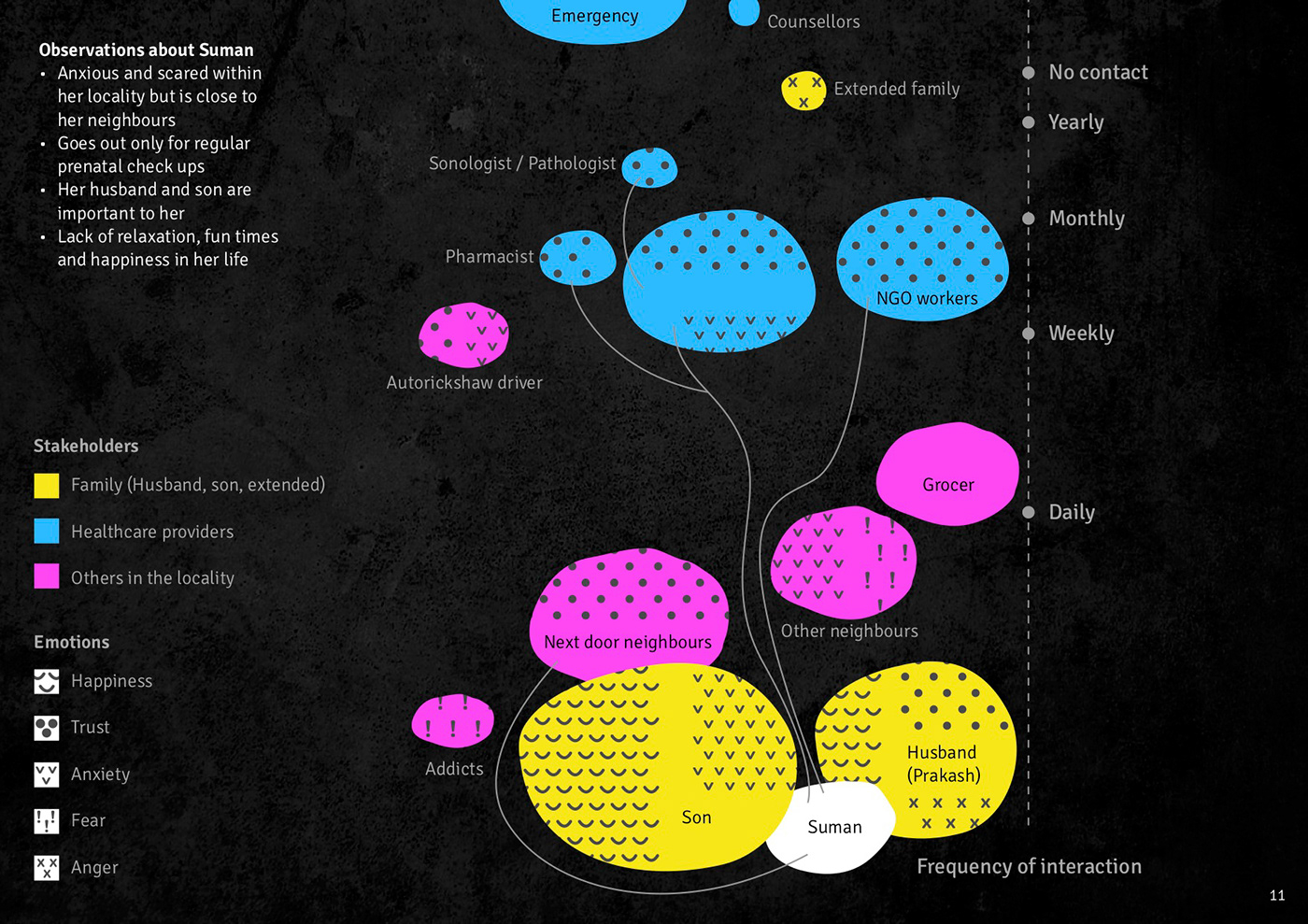
I spoke to a paediatrician, Dr Meenakshi Upadhye, who has worked for more than 25 years in a government-run hospital in a similar area. She shared that the government provides free health services, counselling for disadvantaged people, they pay only for a few select medicines and vaccines. After doing the network map, it was evident that several services are close by and are affordable. Then, why is she still deprived? There’s a need to dig deeper into where her problem actually lies.
Problem space mapping
“Designers tend to use solution conjectures as the means of developing their understanding of the problem. Since the problem cannot be fully understood in isolation from consideration of the solution, it is natural that solution conjectures should be used as a means of helping to explore and understand the problem formulation…They use early solution attempts as experiments to help identify relevant information about the problem.” Nigel Cross. (2007). Designerly Ways of Knowing
I created a 2D image of the problem area using tactile materials. Working with materials gave a lot of freedom with respect to texture, colour, form and properties. It helped me understand that a problem can be represented further by adding the dimension of materials. Each material was chosen based on some inherent quality to suit the corresponding section.


Summary
Current scenario of women like Suman
1. Time and energy get consumed in household chores
2. No time for self, child, relaxation, entertainment
3. Even if she finds time to go out once in a while, the area where she lives is unsafe
4. Has a phone with access to internet. That’s the source of entertainment and connection (Statistics suggest a high consumption of phone internet in the urban poor)
5. She gets a call from the government hospital to remind her about her prenatal check, vaccinations for the child etc, but doesn’t herself keep track
Challenges faced by healthcare providers
1. Huge demand for proper healthcare services in disadvantaged areas because of a very large population to cater to
2. No matter how many government facilities, doctors, nurses, NGO volunteers are working, the help is always inadequate
3. Lack of awareness among women about self-care, health and hygiene especially pre and post-natal
4. Exhaustion due to relentless efforts and yet not close to achieving the optimum goal

Hypotheses
1. A primary assessment of her emotional experiences and problem space got me interested in the role that her neighbours and immediate family play in her life — it’s an intimate relation based on trust and one that gives her happiness.
How might we take the help of her immediate family and people around her to make the experience of her first 1000 days better?
How might we take the help of her immediate family and people around her to make the experience of her first 1000 days better?
2. The network map suggested that several services are close by, affordable or even available free of cost.
How might we change the dynamics of the service by bringing it to her than she coming to the service and what could be the areas of focus?
How might we change the dynamics of the service by bringing it to her than she coming to the service and what could be the areas of focus?
Engagement and Strategy
Two engagement activities were conducted with two different types of stakeholders
Part A — Women (to understand their lived experiences)
Part B — Designers (to brainstorm on ideas)
Part A1
As the primary receiver of the healthcare services, I decided to talk to a few women from disadvantaged families about their experiences of the first 1000 days. I had to keep the discussion simple and lend a listening ear to their stories.
Objective
1. Understand the services, touch points, and support from the stakeholders provided to the woman and her reaction to each of them through the first 1000 days
2. To understand the emotional journey of the woman during pregnancy and post-delivery while interacting with healthcare professionals and family members
3. To capture areas of intervention where the woman has reported unhappiness or irritation
4. Whether the communication between the woman and the stakeholders was effective
Rationale
Pregnancy is a physical journey which is governed by emotions at every stage due to the hormonal changes that happen in the body. Therefore, I wanted to study the different emotions that these women went through in the first 1000 days. I had established her relationship with each stakeholder and their importance in her life. They were doctors, nurses, NGO workers, husband, family, neighbours. This activity was focused on understanding the woman’s interactions with each of the stakeholders and the associated emotions. Overall the women were very happy and confident about facilities provided by the government and NGO support. The problem areas were the lack of support from the husband and the extended family. And therefore the need to reach them through a much more intimate and personal media like a mobile phone.
How did the engagement take place?
I had a one-on-one discussion with three women separately. A set of 28 cards with major events that take place during pregnancy and post-delivery was created. I made a timeline that had events like pregnancy detection, during pregnancy, labour and childbirth, 3 months, 6 months, 12 months, 18 months, 24 months plotted on the X-axis. The Y-axis had emotions such as happy, confident, neutral, confused, unhappy mapped on it. The woman was given the event cards to plot as they happened against the range of emotions. Supporting questions were asked while plotting the cards.


The plotting of cards was digitally created into an emotional journey map for gaining clarity.

Emotional journey map - Participant 1

Emotional journey map - Participant 2
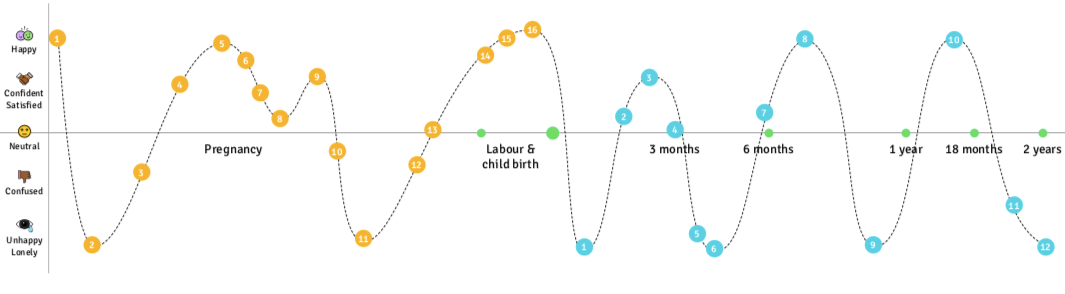
Emotional journey map - Participant 3
Part A2
A common complaint from doctors is that disadvantaged women do not care for their health during pregnancy. Doctors get exhausted explaining basic things over and over again to these women. I wanted to test this through a card selection activity.
Objective
1. To study whether the services were effective in providing information to the woman
2. Her seriousness about taking care of her health and herself
3. Study her usage of mobile phones and whether communicating with her through a mobile phone would be effective
Rationale
The society tends to be more patriarchal in approach, thus women from these families have been told since an early age that their health is unimportant. Awareness levels about taking care of ones health would be very low.
How did the engagement take place?
1. After plotting the emotional journey, a set of 12 cards showing things that are necessary/useful during pregnancy that was created, was shown to the woman
2. She was asked to select from the cards the things she has used or done during her pregnancy


It was true that the women did not treat themselves in any special manner during pregnancy. They knew the dos and don’ts but the effort to stay happy was lacking and no one in the family seemed to care much. I asked them questions while conducting the activities and got a few details related to the ‘why’ behind this behaviour. I also ran a quick Yes/No questionnaire to note their comfort with mobile phone usage. The shared sentiment of all three women was, “I felt relieved after so many years by sharing my story even though it had a few sad memories.”
Part A3
Objective
To understand her mobile phone usage pattern
How did the engagement take place?
A simple Yes/No questionnaire was created



Empathy and objectivity
Pregnancy, childbirth and parenthood is a rollercoaster ride. It comes with its fair share of ups and downs. I was going through the first 1000 days experience myself so, initially, I thought that the experience of other women, even if they belonged to disadvantaged families, would be more or less similar. Little did I know that real-life struggles could be an eye-opener for me at a study level as well as at a personal level. On the upside, I could relate to the journey, since I am a mother myself. This justified the reason why designers use the shadowing technique while conducting research. I understood the importance of a lived experience or an attempt to go as close to it as possible to design engaging activities and solutions even in the future.
Some of the stories involved an alcoholic husband, domestic violence, gender preference for a male child, poor quality of life, financial problems etc. I agree that it is impossible to solve their personal and social problems. Here, I had to take a step back and not get involved emotionally. I had to consider that government policies would play a huge role in achieving success but it would be a very slow process. India has a large population and it’s impossible to work at that scale single-handed. Therefore, the strategy was based around what could be achieved with proportionate effort and have a larger impact, based on a strong insight.
Listening
I communicated with the participants in their language and was able to connect better by asking relevant questions. I tried to make them feel comfortable by respecting their opinions and making them feel that I really cared. The women participants poured their hearts out and shared private details of their parenthood journeys even though I didn’t know them personally. This stood out as the most powerful insight in my entire study that, ‘Everyone needs a listening ear.’ It, therefore, became the central theme of my strategy of connecting these women through mobile phones.
Lack of awareness + Need for social connection + Phone usage with internet + Difficulty in accessing health services = A strong case for a change in the nature of the service provided: increase awareness about pre and post-natal healthcare through a digital platform.
A quantitative survey that answers the above questions would provide more evidence for the proposition and refine it further.
Part B
I had the most fun conducting this activity. I got in touch with a designer friend to have a look at the ideas I had. She readily agreed and also asked if a few of her team members could participate. After a brief discussion, I came back home to design the third engagement activity. We made three sections of chits listing down problems faced by pregnant women, caregivers’ problems and technology and platforms. Picking up the chits at random and finding links between seemingly unrelated things compelled us to think beyond the obvious. The designers were art school students and eager to participate in a new activity. I was satisfied not just with the outcome, but also that we all had a great time coming up with ideas. We also had help from the office helper who works at an NGO for women and children. She was able to provide valuable inputs about how pregnant women from disadvantaged families could be reached to take better care of themselves.
How did the engagement take place?
1. Three sections of chits were made — problems faced by a pregnant woman, pain points of caregivers, technology and digital platforms
2. Each participant was asked to pick a chit from each of the three sections
3. Find a link between the three things picked up at random and come up with a mobile-based idea based on the same. For eg: Remembering health check-up appointments (woman), women don’t take care of themselves (caregivers), phone calendars
4. Collate the results for testing



Idea synthesis
The ideas from the sticky notes were collated into groups corresponding to the women’s pain points.

Going beyond a ‘work’ project to creatively craft approaches to grow the practice
Collating and synthesising the data validated the strategy of leveraging the use of mobile phones to spread awareness about pre and post-natal care among disadvantaged women. The solution had to be easy to execute and scalable.
The Relative prioritization exercise was chosen to compare the solutions based on their reach versus the positive impact on the woman’s life (user value)
India has a lot of diversity with respect to languages, cultures, diet habits, religious beliefs. It became critical that the solution was scalable to appeal to decision-makers — government hospitals and NGOs and at the same time be effective by focusing on adding value to the woman’s needs.

The two selected ideas were then detailed out using a Lean Business Canvas. The Lean Business Canvas was a cohesive way to address the pain points of caregivers and the women, come up with solutions, evaluate commercials and hence provide an objective look at the strategy in one go.
A design strategy should deliver not just on what would be helpful to the user but also address commercial and strategic viability for the government hospitals and NGOs. Considering that the women are from disadvantaged families, it was necessary to consider that they won’t be comfortable to spend on any value-added service.

Idea 1: SMS and messaging
1. Most women share their mobile phone numbers while registering themselves at the government hospital during pregnancy
2. Pregnant women can be sent messages with relevant content via bitly links
3. HTML links will load quickly even in areas where internet connection is low
4. Opportunity to send communication touching several aspects of pregnancy and motherhood, personalised for the woman

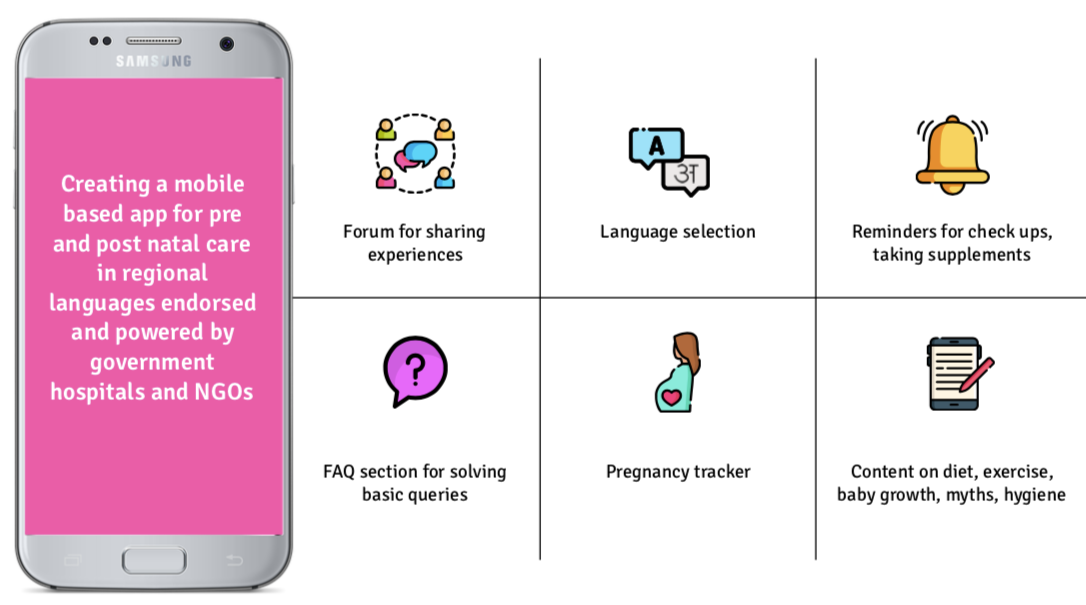
Idea 2: App for pre and post-natal care in regional languages
1. Regional languages will make it more accessible to a large base
2. Can be built by tying up with government hospitals and NGOs
3. Time-consuming and costly to create
I proposed a basic app broadly based on the pain points of caregivers and pregnant women.
Reflection on the research statement
The desirability, viability and feasibility model was used to test whether the solution would have a positive impact on the end-user, caregivers as well as be commercially and technologically possible.
The research statement spoke about leveraging the use of mobile phones to spread awareness about pre and post-natal care among women from disadvantaged areas. The DVF model brought more clarity to the success/failure of the solution and helped build a strong case.

Overall, the idea seems viable, feasible and it delivers on all of the problems from the Lean business canvas
Pros
· Delivers on 4 out of 4 problems
· Quite feasible
· Revenue from advertisers
· Personalised content for women relevant to them
Cons
· Slower internet connections might result into video content loading very slowly
· Special efforts for moderation for the social platform (forums), keeping a track of deleting women from the database who have not continued their pregnancy
· Women might initially find it difficult to share their experiences and some of them may not even download the app
· Additional cost for content creation
· Marketing campaigns to roll out would also mean additional cost
Phase-wise recommendations

Conclusion
In my practice, I like to take a multi-disciplinary approach and apply models from one area to another and see how they impact the decisions that I take as a designer. This methodology has helped me think from different angles and discover more dimensions to the same question. At the same time, I try to come up with tangible solutions even if the problem is ill-defined and ambiguous.
Becoming a mother is probably the best feeling. It shouldn’t get marred by cultural beliefs, social standing and personal limitations. I wish each and every woman would celebrate this experience by feeling confident and happy. One of the ways to do so could be to empower her with knowledge and spread the joy of parenthood.

